
The road to a malaria vaccine for those at risk is reminiscent of a road in rural Africa. Long, rocky and arduous; after every stage that is mastered, the next effort is already waiting. Another interim goal has just been achieved. The Gavi vaccine alliance pledged three-year start-up funding of $ 156 million to launch the world’s first malaria vaccine.
The vaccine with the name Mosquirix or RTS, S was developed in more than 30 years of work; We have known its potential for six years. It can save 30 percent of young children from life-threatening malaria courses. That is a number that, in some cases, still causes worry lines on the faces of those who distribute the chronically scarce funds for global health. 30 percent is far from the optimum. For the Covid vaccines, for example, the World Health Organization (WHO) and some regulatory authorities had required an effectiveness of at least 50 percent, and it was observed that anything below 90 percent only caused a frown in parts of the world.
In the malaria areas, however, the situation is somewhat different. In the green area around Lake Victoria in western Kenya, for example: The Anopheles mosquito thrives here. The residents have always experienced how steadily it transmits the malaria parasites when it stings a person. The pathogens make the little ones especially feverish, vomit and cramp; they can cause anemia, breathing problems, kidney failure, coma, and death.
Tens of thousands of children’s lives could be saved by vaccination.
In the garden of a small ambulance near Luanda, Rose Ayuma, responsible for malaria control in the region, stands under tall trees and loses her composure when the suboptimal 30 percent comes up. “30 percent is a lot!” She calls out more than once. Every year more than a quarter of a million children in Africa die of tropical fever. Vaccination could save tens of thousands of them.
The fear long cherished by the WHO that the vaccination might lead to a false sense of security, so that families forego tried and tested means such as bed nets, is difficult to understand in regions where malaria is widespread. As if the people here didn’t know that infectious diseases – whether malaria or Covid-19 – can be combated with a whole arsenal of options. “The malaria vaccination is our booster,” says Rose Ayuma.

This ambulance near Luanda was one of the centers where the feasibility of the malaria vaccination was tested. The conditions weren’t easy.
(Photo: Global Fund)
For many who have their little house here, the question of bed nets is more academic anyway. Just under 60 percent of children under five in the Lake Victoria area regularly sleep under a net impregnated with insecticides, according to a survey by the Kenyan government last year. In the villages around Luanda, too, people were only given the protective nets last summer. The malaria vaccinations had long since started.
The area near the lake is one of around 180 regions in Africa in which the WHO is having a feasibility study tested to determine whether the effort of the malaria vaccination – four injections in the first two years of life – can actually be managed. Since September 2019, helpers have been moving through the villages to inform the mothers about the new vaccination. In the scorching heat they walk across the red earth on paths that have no name to houses that have no address. They covered kilometer by kilometer – even when the corona pandemic began and the fear of the new virus was as great as the lack of protective equipment, they continued.
So far, the helpers have sent around 200 children to the outpatient clinic near Luanda for the malaria vaccination. Eunice Vugutsa, an employee of the facility, opens the big black book in which all the vaccination doses that were administered here are noted in fine handwriting. The feasibility study receives worldwide attention, the final results are likely to appear in a prominent journal – scientific excellence in high gloss. And yet here in the low building between acacias and guavas there isn’t even a computer for data collection.
Most ambulance workers barely earn enough to feed their families.
Eunice Vugutsa laughs: Computers are generally not intended for the small outpatient clinics that provide basic care. In their facility, the water has to be brought in plastic tubs. The toilets are a hole in the floor, surrounded by a rickety wooden crate. Most employees barely earn enough to support their families. And yet they managed to administer the first three doses of the malaria vaccine even during the corona pandemic. The immunizations were steady and reliable, as can be seen when Eunice Vugutsa runs her finger down the cracks in the book. The other study regions also managed to administer the first three doses, according to the interim conclusion of the WHO, which is why the authority recommended the vaccine for all children at risk at the beginning of October. Not enough data were initially available for the fourth dose.
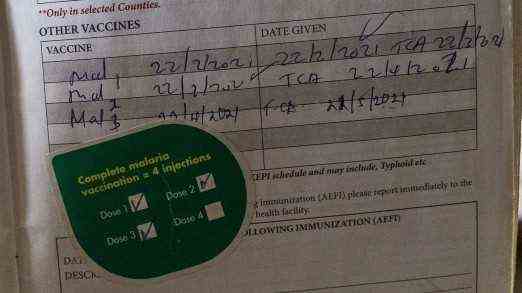
The first three doses of the vaccine were given reliably. The fourth is currently showing difficulties.
(Photo: Global Fund)
However, it is precisely for this dose that the data collection of the small ambulance shows worrying figures. Only about a third of all children whose vaccination appointment was due received this last injection. Whether this is just a momentary delay or an indication of a major problem remains to be seen. In any case, the employees are worried – especially about those families who have moved away in the meantime. If their new home is not in one of the study areas, the children will miss the last dose for an uncertain time – and thus significantly reduce their protection. This is one of the reasons why the employees here hope so much that the vaccine will quickly be used across the board. Especially since more and more families from neighboring districts are coming to them who also want malaria protection from the syringe for their children.
But when children outside of the study can also receive the vaccine is still completely open. “It is difficult to say when the first deliveries will take place,” said Gavi. First of all, there are a number of other steps to be taken: the vaccine has to be procured, vaccination programs have to be planned. The federal states have to submit applications for funding, for which an application procedure has to be drawn up in the first place.
And it is already questionable how long the money and vaccines will last. “The initial supply of the RTS, S vaccine may not be enough to meet potential demand in the medium term,” says Ashley Birkett, director of vaccine development at Path, a non-governmental organization that promotes new malaria vaccines, among other things. Because unlike the Covid vaccines, the international community did not invest in the timely expansion of vaccine production in the case of malaria.
Saschveen Singh, consultant for tropical diseases at the organization Doctors Without Borders, criticized “the currently unacceptably long periods of time” for the introduction of the vaccine. He called on Gavi to speed up the processes and to give countries with the weakest health systems additional support to set up a vaccination program.
The road to a malaria vaccine for all children remains long and rocky.
The research for this text was partly funded by the Global Fund to Fight AIDS, Tuberculosis and Malaria.