
Doctors have declared the Government’s push to reclassify marijuana as a less dangerous drug, a ‘political move that goes against science’ and ‘glosses over’ serious risks of addiction and psychosis.
The Drug Enforcement Agency (DEA) is announced plans to downgrade marijuana from a schedule one substance to schedule three, putting it in the same safety category as some types of Tylenol and steroids.
If the rule is officially adopted, marijuana will be considered less risky than LSD, ecstacy, codeine, Adderall and cocaine. It would be the agency’s biggest policy change in 50 years, though it would not outright legalize the drug.
However, medical experts told DailyMail.com that reclassifying cannabis could mislead the public into believing the drug is safe, and dismiss serious risks like addiction, heart disease, and severe psychiatric illness.
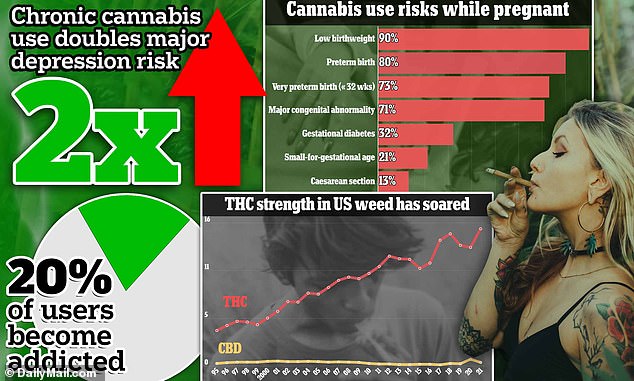
There is particular concern about the impact of mind-altering high-potency marijuana that dominates the market today, with levels of psychoactive THC around 13-15 percent, on average. In the 1970s, the average joint contained around two to four percent THC.

Emily Rose Perrin, who suffered cystic fibrosis, was suffocated and killed by her mother who is believed to have been experiencing psychiatric illness related to cannabis use

Kiaire McCoy got hold of his mother’s ex-boyfriend’s loaded gun and shot himself earlier this year. The gun owner was supposed to be watching Kiaire but ‘zoned out’ while high on marijuana
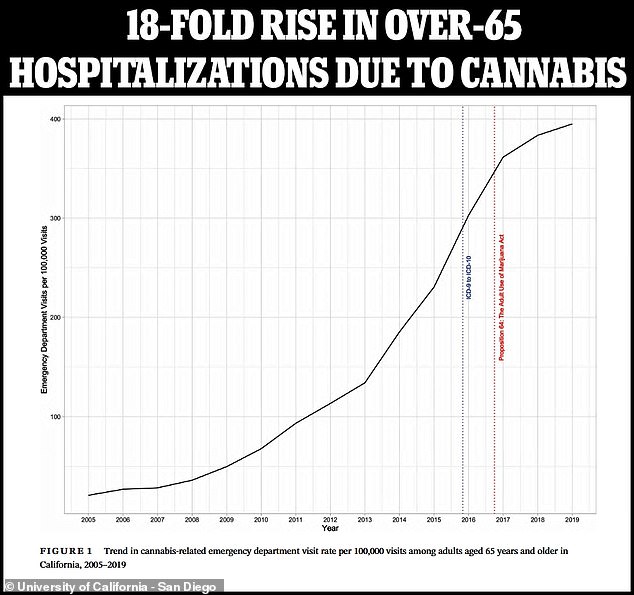
Data suggests weed-related addiction, mental illness, and hospitalization, have soared in states like California where recreational cannabis has been legalized.
The drug has also been blamed for hundreds of child deaths due to parents ignoring their responsibilities while high, or entering a dangerous psychosis.
And earlier this year, the case of Bryn Spejcher, a 32-year-old audiologist who went into a weed-induced psychosis and stabbed her boyfriend over 100 times, thrust the harms of cannabis into the spotlight.
Dr Roneet Lev, an emergency medicine physician and addiction specialist at Scripps Mercy Hospital in San Diego, told DailyMail.com: ‘This is a sad day for the children of America who are being exposed to more of this.’
‘We’re not following the science and it’s right there in front of us.’
However, official death data shows the number of fatalities related to the drug remain low, at around 300 a year, compared to roughly 10,000 from schedule one heroin.
What’s more, the DEA says there are no annual deaths from marijuana overdoses.
But is it really less dangerous than ecstasy, cocaine, codeine and Adderall?

Bryn Spejcher, a 32-year-old audiologist in California, went into violent psychosis after smoking marijuana, which she was normally against. She stabbed her boyfriend 108 times, as well as herself and her beloved dog
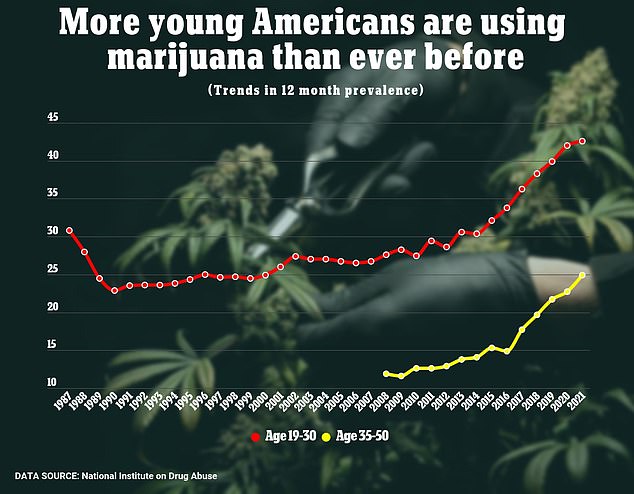
Federal research has shown that cannabis use is growing, particularly in Americans under the age of 30
Recent CDC figures suggest perhaps not, when it comes to hospitalizations. Between December 30, 2018, and January 1, 2023, there were nearly 540,000 ER visits related to cannabis.
In comparison, there’s around 3,200 visits per year for MDMA (or ecstasy) – 56 times fewer than those related to weed.
Most of these admissions are related to the psychiatric effects of marijuana.
One study published last year found that regular cannabis users were more than twice as likely to suffer serious psychological distress than those who did not use weed.
What’s more, one 2019 UK study found that those who smoked high-potency marijuana were five times more likely to develop psychosis. There have also been anecdotal reports of high-potency marijuana vapes linked to psychotic breaks, suicidal thoughts, and deaths by suicide.
Scientists believe that the THC in cannabis interferes with signals in the brain that contol mood, attention and memory, as well as feelings of reward and pleasure.
The DEA classifies drugs into five categories based on how likely they are to be abused. Schedule one drugs, which marijuana currently falls under, have the highest chance of abuse and ‘the potential to create severe psychological and/or physical dependence.
Other schedule one drugs include heroin, LSD, ecstacy, and MDMA.
Schedule two drugs include cocaine, methamphetamine, oxycodone, fentanyl, and Adderall. Meanwhile, current schedule three drugs are ketamine, some anabolic steroids, and testosterone.
Schedule four includes Xanax, Valium, and Ambien, among others, and the least dangerous, schedule five, include cough medicines with less than 200 miligrams of codeine, such as robitussin AC, and the arthritis medicine Lyrica.
Schedule three drugs are still controlled substances and subject to rules and regulations, and people who traffic in them without permission could still face federal criminal prosecution.
Researchers have noted that drugs in Schedule one have no medicinal benefits, while scheduling marijuana down acknowledges that it has some medical uses.
But experts say addiction is a common issue with marijuana – it just often flies under the radar.
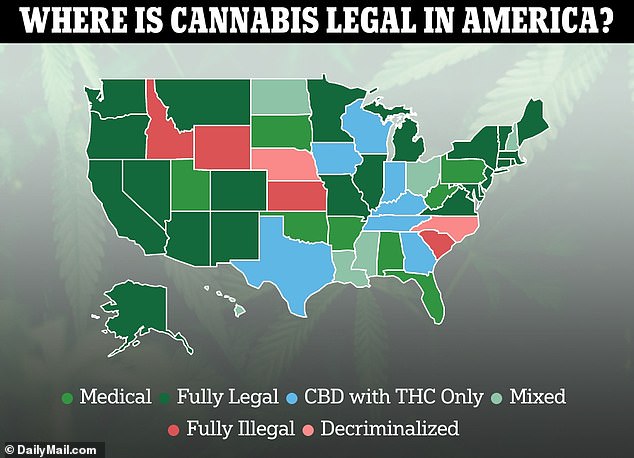
Recreational marijuana is legal in 24 states, though others have legalized it only for medicinal purposes
Scientists have a hard time agreeing on where the addiction threshold is for marijuana, but studies estimate about four million Americans qualified as having a ‘marijuana use disorder’ in 2015, according to the National Institute on Drug Abuse (NIDA).
That group accounts for about nine percent of all marijuana-users. But addiction rates nearly doubled – rising to 17 percent – among people that started getting high in their teenage years.
Additionally, a study in Journal of Clinical Psychiatry found that nearly one in five people who smoke cannabis met the criteria for dependence.
Dr Lev noted that the addiction rate ‘could be as high as 50 percent’ for those who stasrt using at young ages and opting for potency above 10 percent THC.
Other mental health risks of regular cannabis use has also been shown in studies. Danish researchers delved into the records of more than 6.6 million people in Denmark born between 1985 and 2021 and found of those addicted to cannabis, about 41 percent of those individuals were diagnosed with major depression.
They also found chronic marijuana use quadrupled a person’s risk of being diagnosed with bipolar disorder.
Other drugs in Schedule one have similar effects. One review found that heavy use of MDMA, for example, may inhibit the production of serotonin, decreasing mood and sense of pleasure.
Additional research has found that long-term LSD use can trigger psychosis and schizophrenia in some users.
Recent research has shed light on marijuana’s risk to physical health. A study of 400,000 adults published in the Journal of the American Heart Association, for example, found that any type of cannabis use was ‘associated with a higher number of adverse cardiovascular outcomes.’
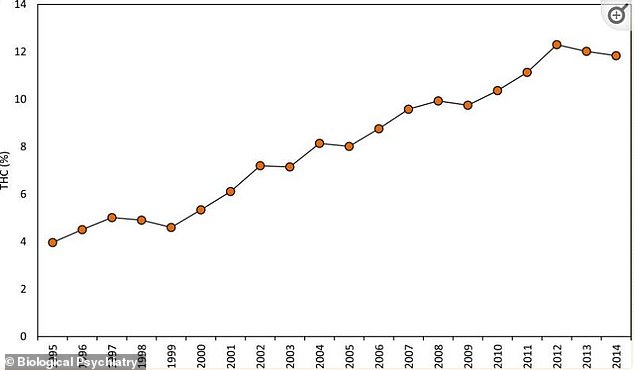
The strength of cannabis has increased exponentially in recent decades
This included daily weed users having a 25 percent higher risk of heart attack and a 42 percent increased chance of suffering a stroke.
Additionally, research from November found that adults over 54 years old who smoked marijuana daily had a 34 percent higher risk of heart failure.
An accompanying study researchers found hospitalized people over 65 years old who had used marijuana — but not cigarettes — were 20 percent more likely to suffer a major heart event or stroke.
Researchers warned data was ‘strongly pointing’ to the fact that ‘cannabis use at any point in time, be it recreational or medicinal,’ was not without risks.
There is little concrete data on deaths directly caused by marijuana and some Schedule one drugs like LSD and MDMA, though the estimates are small compared to drugs like cocaine.
While marijuana death estimates range from about 100 to 300 per year, a CDC report found that between 2019 and 2012, there were 24,486 deaths from cocaine overdose. This was a 54 percent increase from 2015 to 2019.
The rates of hospitalization due to marijuana, meanwhile, are staggering.
Research from 2022, for example, suggested that recreational marijuana users were 25 percent more likely to end up needing emergency hospital treatment. And, according to data from the US Fatality Analysis Reporting System, the risk of being involved in a cannabis-related accident is significantly higher in states where the drug is legal.
Additionally, the CDC reported that between December 30, 2018, and January 1, 2023, there were nearly 540,000 cannabis-involved emergency room visits among people under 25 years old.
Data from a 2021 Substance Abuse and Mental Health Services Administration (SAMHSA) report found over 787,000 emergency room visits due to marijuana, most of which – 45.2 percent – were among those ages 26 to 44.
This was similar to ED visits for methamphetamine use, which totaled nearly 800,000. These include ADHD medications like Adderall.
Dr Lev noted that lowering the classification could give users the false impression that consuming marijuana is harmless, when research paints a more grim picture.
However, not all experts agree that re-classifying cannabis is a bad idea.
Dr Anna Lembke, a professor of psychiatry at the Stanford University School of Medicine, told DailyMail.com that ‘cannabis is clearly addictive’ but said that rescheduling marijuana acknowledges that it has some medicinal benefits as well.
‘I think it’s a good move,’ she said. This is because schedule one drugs cannot be federally researched, except by few institutions, leading to inconsistent data about the risks and benefits.
‘Putting it into schedule three makes it possible for researchers to gather robust clinical data to see what the use cases are, including its medical efficacy for various conditions, as well as risks, benefits, and alternatives,’ Dr Lembke said.
She noted marijuana being a schedule one drug has led to poorly designed studies with flawed methodology and only short-term design, which gives the public a skewed perspective.
‘Right now what we have is a lot of poorly done studies on cannabis making it difficult to know what to tell patients about cannabis available at their local state dispensary,’ she said.
Dr Lembke said she hopes the rescheduling leads to additional data and ultimately the FDA approval of some forms of cannabis rather than leaving it up to the states.
‘All we have right now is a hodgepodge system at the state level with varying degrees of oversight and regulation, and no robust evidence base for when and how to use it.’
‘Cannabis is clearly addictive. And is also clearly has medicinal properties, at least when used short term. So we need to figure out how so we can use it for its medicinal properties but also make sure that we protect people from the adverse consequences, including the very strong potential for addiction.’
Dr Lev noted that while she doesn’t discourage people from using cannabis, there is currently not enough evidence on the risks for benefits for people to know exactly what they’re getting into.
‘We aren’t telling people to not use but to make an informed decision, and right now we have an ill informed public,’ she said.
‘People need to be making informed decisions, and marijuana is not at that point in terms of public health information.’